- 4,780
- 5,114
- Joined
- Jul 29, 2012
Follow along with the video below to see how to install our site as a web app on your home screen.
Note: this_feature_currently_requires_accessing_site_using_safari
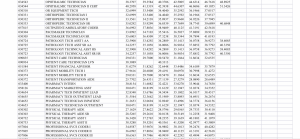
cracks me up when "physicians" think they got all the answersINFORMATION FOR PATIENTS — UpToDate offers two types of patient education materials, "The Basics" and "Beyond the Basics." The Basics patient education pieces are written in plain language, at the 5th to 6th grade reading level, and they answer the four or five key questions a patient might have about a given condition. These articles are best for patients who want a general overview and who prefer short, easy-to-read materials. Beyond the Basics patient education pieces are longer, more sophisticated, and more detailed. These articles are written at the 10th to 12th grade reading level and are best for patients who want in-depth information and are comfortable with some medical jargon.
Here are the patient education articles that are relevant to this topic. We encourage you to print or e-mail these topics to your patients. (You can also locate patient education articles on a variety of subjects by searching on "patient info" and the keyword(s) of interest.)
●Basics topics (see "Patient education: HIV/AIDS (The Basics)" and "Patient education: Tests to monitor HIV (The Basics)")
SUMMARY
●Human immunodeficiency virus (HIV) infection can be divided into the following stages: viral transmission, acute HIV infection with seroconversion, and chronic HIV infection with or without evidence of the acquired immunodeficiency syndrome (AIDS). (See 'Overview of stages of HIV infection' above.)
●HIV infection is usually acquired through sexual intercourse, exposure to contaminated blood, or perinatal transmission. Risk factors for transmission include high viral load, certain sexual behaviors, presence of ulcerative sexually transmitted infections (STIs), lack of circumcision, and certain host and genetic factors. (See 'Viral transmission' above.)
●Symptomatic acute HIV infection is characterized by fever, lymphadenopathy, sore throat, rash, myalgia/arthralgia, and headache; however, a substantial proportion of patients with early HIV infection are asymptomatic. Early HIV infection is a period of rapid viral replication with typically very high viral RNA levels. By approximately six months of infection, plasma viremia has reached a steady state level. (See 'Acute and early HIV infection' above and "Acute and early HIV infection: Clinical manifestations and diagnosis".)
●The period of chronic HIV infection following early infection and seroconversion but prior to the development of severe immunosuppression is characterized by relative stability of viral levels and a progressive decline in CD4 cell count. The rate of CD4 cell decline correlates with the level of viremia. During this stage, the majority of HIV-infected patients are asymptomatic, although some may have generalized lymphadenopathy. However, certain HIV-associated clinical findings, such as thrush, seborrheic dermatitis, and susceptibility to herpesvirus and human papillomavirus (HPV) infections, bacterial pneumonia, and tuberculosis, frequently occur despite a CD4 cell count >200 cells/microL. (See 'Chronic HIV infection, without AIDS' above.)
●AIDS is defined by a CD4 cell count <200 cells/microL or the presence of any AIDS-defining condition (table 5) regardless of the CD4 cell count. (See 'AIDS and advanced HIV infection' above.)
●AIDS-defining conditions are opportunistic illnesses that occur more frequently or more severely in immunocompromised hosts. These include mainly opportunistic infections, such as Pneumocystis jirovecii pneumonia, toxoplasmosis, and disseminated Mycobacterium avium infection. Certain malignancies (Kaposi sarcoma, lymphoma), as well as conditions without clear alternative etiology thought to be related to uncontrolled HIV infection itself, such as wasting or encephalopathy, are also AIDS-defining conditions. (See 'AIDS defining conditions' above.)
●A minority of HIV-infected patients, despite not being on antiretroviral therapy (ART), has very low levels of viremia. They are considered HIV controllers. A subset of these patients are referred to as non-viremic controllers because they have no detectable viremia, even on ultrasensitive diagnostic testing. (See 'HIV controllers' above.)
●HIV-1 causes the vast majority of HIV infections worldwide, although HIV-2 is an important cause of infection in certain regions of the world, such as West Africa. Compared with HIV-1, HIV-2 infection is characterized by lower levels of plasma virus, slower declines in the CD4 cell count, and a longer asymptomatic period of chronic infection. (See "Epidemiology, transmission, natural history, and pathogenesis of HIV-2 infection" and "Clinical manifestations and diagnosis of HIV-2 infection" and "Treatment of HIV-2 infection".)
ACKNOWLEDGMENT — The editorial staff at UpToDate would like to acknowledge John G Bartlett, MD, who contributed to an earlier version of this topic review.
Use of UpToDate is subject to the Subscription and License Agreement.
REFERENCES
- Mocroft A, Ledergerber B, Katlama C, et al. Decline in the AIDS and death rates in the EuroSIDA study: an observational study. Lancet 2003; 362:22.
- Samji H, Cescon A, Hogg RS, et al. Closing the gap: increases in life expectancy among treated HIV-positive individuals in the United States and Canada. PLoS One 2013; 8:e81355.
- Centers for Disease Control and Prevention (CDC). Revised surveillance case definition for HIV infection--United States, 2014. MMWR Recomm Rep 2014; 63:1.
- World Health Organization. WHO case definitions of HIV for surveillance and revised clinical staging and immunologic classification of HIV-related disease in adults and children. World Health Organization, Geneva, Switzerland, 2007, 1-48.
- Adler MW. ABC of Aids: Development of the epidemic. BMJ 2001; 322:1226.
- Quinn TC, Wawer MJ, Sewankambo N, et al. Viral load and heterosexual transmission of human immunodeficiency virus type 1. Rakai Project Study Group. N Engl J Med 2000; 342:921.
- Gray RH, Wawer MJ, Brookmeyer R, et al. Probability of HIV-1 transmission per coital act in monogamous, heterosexual, HIV-1-discordant couples in Rakai, Uganda. Lancet 2001; 357:1149.
- Dorak MT, Tang J, Penman-Aguilar A, et al. Transmission of HIV-1 and HLA-B allele-sharing within serodiscordant heterosexual Zambian couples. Lancet 2004; 363:2137.
- Wawer MJ, Gray RH, Sewankambo NK, et al. Rates of HIV-1 transmission per coital act, by stage of HIV-1 infection, in Rakai, Uganda. J Infect Dis 2005; 191:1403.
- Buchbinder SP, Vittinghoff E, Heagerty PJ, et al. Sexual risk, nitrite inhalant use, and lack of circumcision associated with HIV seroconversion in men who have sex with men in the United States. J Acquir Immune Defic Syndr 2005; 39:82.
- Pilcher CD, Fiscus SA, Nguyen TQ, et al. Detection of acute infections during HIV testing in North Carolina. N Engl J Med 2005; 352:1873.
- Bailey RC, Moses S, Parker CB, et al. Male circumcision for HIV prevention in young men in Kisumu, Kenya: a randomised controlled trial. Lancet 2007; 369:643.
- Gray RH, Kigozi G, Serwadda D, et al. Male circumcision for HIV prevention in men in Rakai, Uganda: a randomised trial. Lancet 2007; 369:657.
- Gray R, Kigozi G, Kong X, et al. The effectiveness of male circumcision for HIV prevention and effects on risk behaviors in a posttrial follow-up study. AIDS 2012; 26:609.
- Auvert B, Taljaard D, Lagarde E, et al. Randomized, controlled intervention trial of male circumcision for reduction of HIV infection risk: the ANRS 1265 Trial. PLoS Med 2005; 2:e298.
- Baeten JM, Donnell D, Kapiga SH, et al. Male circumcision and risk of male-to-female HIV-1 transmission: a multinational prospective study in African HIV-1-serodiscordant couples. AIDS 2010; 24:737.
- Fiebig EW, Wright DJ, Rawal BD, et al. Dynamics of HIV viremia and antibody seroconversion in plasma donors: implications for diagnosis and staging of primary HIV infection. AIDS 2003; 17:1871.
- Branson BM, Stekler JD. Detection of acute HIV infection: we can't close the window. J Infect Dis 2012; 205:521.
- Branson BM, Ginocchio CC. Introduction to 2013 Journal of Clinical Virology supplement on HIV testing algorithms. J Clin Virol 2013; 58 Suppl 1:e1.
- Pedersen C, Lindhardt BO, Jensen BL, et al. Clinical course of primary HIV infection: consequences for subsequent course of infection. BMJ 1989; 299:154.
- Niu MT, Stein DS, Schnittman SM. Primary human immunodeficiency virus type 1 infection: review of pathogenesis and early treatment intervention in humans and animal retrovirus infections. J Infect Dis 1993; 168:1490.
- Pantaleo G, Demarest JF, Schacker T, et al. The qualitative nature of the primary immune response to HIV infection is a prognosticator of disease progression independent of the initial level of plasma viremia. Proc Natl Acad Sci U S A 1997; 94:254.
- Musey L, Hughes J, Schacker T, et al. Cytotoxic-T-cell responses, viral load, and disease progression in early human immunodeficiency virus type 1 infection. N Engl J Med 1997; 337:1267.
- Mellors JW, Kingsley LA, Rinaldo CR Jr, et al. Quantitation of HIV-1 RNA in plasma predicts outcome after seroconversion. Ann Intern Med 1995; 122:573.
- Lavreys L, Baeten JM, Chohan V, et al. Higher set point plasma viral load and more-severe acute HIV type 1 (HIV-1) illness predict mortality among high-risk HIV-1-infected African women. Clin Infect Dis 2006; 42:1333.
- Schacker TW, Hughes JP, Shea T, et al. Biological and virologic characteristics of primary HIV infection. Ann Intern Med 1998; 128:613.
- Madec Y, Boufassa F, Porter K, et al. Spontaneous control of viral load and CD4 cell count progression among HIV-1 seroconverters. AIDS 2005; 19:2001.
- Osmond D, Chaisson R, Moss A, et al. Lymphadenopathy in asymptomatic patients seropositive for HIV. N Engl J Med 1987; 317:246.
- Sterling, T and Chaisson, R. General clinical manifestations of Human Immunodeficiency Virus infection (including the acute antiretroviral syndrome and oral, cutaneous, renal, ocular, metabolic, and cardiac diseases). In: Principles and Practice of Infectious Diseases, 7, Mandell GL, Bennet JE, and Dolin R (Eds), 2010. p.1705.
- Farizo KM, Buehler JW, Chamberland ME, et al. Spectrum of disease in persons with human immunodeficiency virus infection in the United States. JAMA 1992; 267:1798.
- Popovich KJ, Hota B, Aroutcheva A, et al. Community-associated methicillin-resistant Staphylococcus aureus colonization burden in HIV-infected patients. Clin Infect Dis 2013; 56:1067.
- Zervou FN, Zacharioudakis IM, Ziakas PD, et al. Prevalence of and risk factors for methicillin-resistant Staphylococcus aureus colonization in HIV infection: a meta-analysis. Clin Infect Dis 2014; 59:1302.
- Wei X, Ghosh SK, Taylor ME, et al. Viral dynamics in human immunodeficiency virus type 1 infection. Nature 1995; 373:117.
- Ho DD, Neumann AU, Perelson AS, et al. Rapid turnover of plasma virions and CD4 lymphocytes in HIV-1 infection. Nature 1995; 373:123.
- Henrard DR, Phillips JF, Muenz LR, et al. Natural history of HIV-1 cell-free viremia. JAMA 1995; 274:554.
- Pantaleo G, Graziosi C, Demarest JF, et al. HIV infection is active and progressive in lymphoid tissue during the clinically latent stage of disease. Nature 1993; 362:355.
- Henrich TJ, Hanhauser E, Marty FM, et al. Antiretroviral-free HIV-1 remission and viral rebound after allogeneic stem cell transplantation: report of 2 cases. Ann Intern Med 2014; 161:319.
- Gottlieb GS, Sow PS, Hawes SE, et al. Equal plasma viral loads predict a similar rate of CD4+ T cell decline in human immunodeficiency virus (HIV) type 1- and HIV-2-infected individuals from Senegal, West Africa. J Infect Dis 2002; 185:905.
- Touloumi G, Pantazis N, Pillay D, et al. Impact of HIV-1 subtype on CD4 count at HIV seroconversion, rate of decline, and viral load set point in European seroconverter cohorts. Clin Infect Dis 2013; 56:888.
- Mlisana K, Werner L, Garrett NJ, et al. Rapid disease progression in HIV-1 subtype C-infected South African women. Clin Infect Dis 2014; 59:1322.
- Stein DS, Korvick JA, Vermund SH. CD4+ lymphocyte cell enumeration for prediction of clinical course of human immunodeficiency virus disease: a review. J Infect Dis 1992; 165:352.
- Lodi S, Phillips A, Touloumi G, et al. Time from human immunodeficiency virus seroconversion to reaching CD4+ cell count thresholds <200, <350, and <500 Cells/mm³: assessment of need following changes in treatment guidelines. Clin Infect Dis 2011; 53:817.
- Schacker T, Collier AC, Hughes J, et al. Clinical and epidemiologic features of primary HIV infection. Ann Intern Med 1996; 125:257.
- Simon V, Ho DD, Abdool Karim Q. HIV/AIDS epidemiology, pathogenesis, prevention, and treatment. Lancet 2006; 368:489.
- Galai N, Vlahov D, Margolick JB, et al. Changes in markers of disease progression in HIV-1 seroconverters: a comparison between cohorts of injecting drug users and homosexual men. J Acquir Immune Defic Syndr Hum Retrovirol 1995; 8:66.
- Lang W, Perkins H, Anderson RE, et al. Patterns of T lymphocyte changes with human immunodeficiency virus infection: from seroconversion to the development of AIDS. J Acquir Immune Defic Syndr 1989; 2:63.
- Margolick JB, Muñoz A, Vlahov D, et al. Changes in T-lymphocyte subsets in intravenous drug users with HIV-1 infection. JAMA 1992; 267:1631.
- Hughes MD, Stein DS, Gundacker HM, et al. Within-subject variation in CD4 lymphocyte count in asymptomatic human immunodeficiency virus infection: implications for patient monitoring. J Infect Dis 1994; 169:28.
- Moir S, Malaspina A, Pickeral OK, et al. Decreased survival of B cells of HIV-viremic patients mediated by altered expression of receptors of the TNF superfamily. J Exp Med 2004; 200:587.
- Moir S, Malaspina A, Ogwaro KM, et al. HIV-1 induces phenotypic and functional perturbations of B cells in chronically infected individuals. Proc Natl Acad Sci U S A 2001; 98:10362.
- Greene M, Covinsky KE, Valcour V, et al. Geriatric Syndromes in Older HIV-Infected Adults. J Acquir Immune Defic Syndr 2015; 69:161.
- Aberg JA. Aging, inflammation, and HIV infection. Top Antivir Med 2012; 20:101.
- Jones JL, Hanson DL, Dworkin MS, et al. Surveillance for AIDS-defining opportunistic illnesses, 1992-1997. MMWR CDC Surveill Summ 1999; 48:1.
- Hanson DL, Chu SY, Farizo KM, Ward JW. Distribution of CD4+ T lymphocytes at diagnosis of acquired immunodeficiency syndrome-defining and other human immunodeficiency virus-related illnesses. The Adult and Adolescent Spectrum of HIV Disease Project Group. Arch Intern Med 1995; 155:1537.
- Taylor JM, Sy JP, Visscher B, Giorgi JV. CD4+ T-cell number at the time of acquired immunodeficiency syndrome. Am J Epidemiol 1995; 141:645.
- Karon JM, Buehler JW, Byers RH, et al. Projections of the number of persons diagnosed with AIDS and the number of immunosuppressed HIV-infected persons--United States, 1992-1994. MMWR Recomm Rep 1992; 41:1.
- Freedberg KA, Malabanan A, Samet JH, Libman H. Initial assessment of patients infected with human immunodeficiency virus: the yield and cost of laboratory testing. J Acquir Immune Defic Syndr 1994; 7:1134.
- Yarchoan R, Venzon DJ, Pluda JM, et al. CD4 count and the risk for death in patients infected with HIV receiving antiretroviral therapy. Ann Intern Med 1991; 115:184.
- Phillips AN, Elford J, Sabin C, et al. Immunodeficiency and the risk of death in HIV infection. JAMA 1992; 268:2662.
- Easterbrook PJ, Emami J, Moyle G, Gazzard BG. Progressive CD4 cell depletion and death in zidovudine-treated patients. J Acquir Immune Defic Syndr 1993; 6:927.
- Hsue PY, Hunt PW, Schnell A, et al. Role of viral replication, antiretroviral therapy, and immunodeficiency in HIV-associated atherosclerosis. AIDS 2009; 23:1059.
- Pereyra F, Lo J, Triant VA, et al. Increased coronary atherosclerosis and immune activation in HIV-1 elite controllers. AIDS 2012; 26:2409.
- Pereyra F, Palmer S, Miura T, et al. Persistent low-level viremia in HIV-1 elite controllers and relationship to immunologic parameters. J Infect Dis 2009; 200:984.
- Dinoso JB, Kim SY, Siliciano RF, Blankson JN. A comparison of viral loads between HIV-1-infected elite suppressors and individuals who receive suppressive highly active antiretroviral therapy. Clin Infect Dis 2008; 47:102.
- Migueles SA, Connors M. Long-term nonprogressive disease among untreated HIV-infected individuals: clinical implications of understanding immune control of HIV. JAMA 2010; 304:194.
- Klein MR, Miedema F. Long-term survivors of HIV-1 infection. Trends Microbiol 1995; 3:386.
- Migueles SA, Osborne CM, Royce C, et al. Lytic granule loading of CD8+ T cells is required for HIV-infected cell elimination associated with immune control. Immunity 2008; 29:1009.
- Sedaghat AR, Rastegar DA, O'Connell KA, et al. T cell dynamics and the response to HAART in a cohort of HIV-1-infected elite suppressors. Clin Infect Dis 2009; 49:1763.
- Leon A, Perez I, Ruiz-Mateos E, et al. Rate and predictors of progression in elite and viremic HIV-1 controllers. AIDS 2016; 30:1209.
- Walker BD. Elite control of HIV Infection: implications for vaccines and treatment. Top HIV Med 2007; 15:134.
- Pereyra F, Addo MM, Kaufmann DE, et al. Genetic and immunologic heterogeneity among persons who control HIV infection in the absence of therapy. J Infect Dis 2008; 197:563.
I’m not “anti doctor” but I’ve seen plenty of cases where they’ve destroyed kids with medications. Sad and irreversiblecracks me up when "physicians" think they got all the answers
all doctors are
are folks who memorized a damn textbook
anyone can memorize a textbook and become a doctor
doctors think they so smart
i work in the medical field
and have met plenty of idiot doctors
who are dumb as a bag of rocks
When one of your kids are sick, who do you seek help from?cracks me up when "physicians" think they got all the answers
all doctors are
are folks who memorized a damn textbook
anyone can memorize a textbook and become a doctor
doctors think they so smart
i work in the medical field
and have met plenty of idiot doctors
who are dumb as a bag of rocks
mind u
does take a lot of work to be a doctor
but again
they just all memorizing a damn book
Yup. I respect anyone who’s really good at what they do no matter what it is.You could boil any person of any profession down to "someone who just memorized stuff"
If you want to keep it real
I spoke their language and cited the credentials that they usually would to validate their point of view.I should've just posted this from the jump and left it at that.cracks me up when "physicians" think they got all the answers
all doctors are
are folks who memorized a damn textbook
anyone can memorize a textbook and become a doctor
doctors think they so smart
i work in the medical field
and have met plenty of idiot doctors
who are dumb as a bag of rocks
mind u
does take a lot of work to be a doctor
but again
they just all memorizing a damn book
You could boil any person of any profession down to "someone who just memorized stuff"
If you want to keep it real

I’m not “anti doctor” but I’ve seen plenty of cases where they’ve destroyed kids with medications. Sad and irreversible
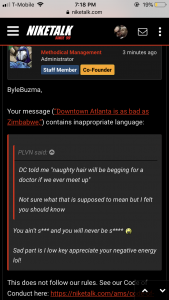
The Perth Group is a group of HIV/AIDS denialists based in Perth, Western Australia who claim, in opposition to the scientific consensus, that the existence of HIV (Human Immunodeficiency Virus) is not proven, and that AIDS and all the "HIV" phenomena are caused by changes in cellular redox due to the oxidative nature of substances and exposures common to all the AIDS risk groups, and are caused by the cell conditions used in the "culture" and "isolation" of "HIV".[1]
The group's activism has negatively affected the epidemic of HIV/AIDS in South Africa due to their influence on the AIDS policies of South African President Thabo Mbeki. The resulting governmental refusal to provide effective anti-HIV treatment in South Africa has been blamed for hundreds of thousands of premature AIDS-related deaths in South Africa.[2]
I tell parents it takes years to build skills but it lasts a life time. TRY first. You can put kids on meds in an instant and after that reaching “normal” just never happens. It’s a horrible cycle. I’m not against meds but WAIT.I was talking about this the other day. Despite genetic parental history increasing ADHD risk, some parents just cant properly raise or discipline children. I have parents who demand their child's Adderall, Concerta, Ritalin, etc. ADHD medications are so damn overprescribed in white male children under 12 years old its unbelievable. If you read in between the lines, the DSM-5 criteria are basically a combination of children who....
-lose focus in school
-dont wait their turn to get called on
-talk excessively
-have sloppy handwriting
-need to be constantly reminded of things
You can argue that that's pretty much a majority of children. Hell that was all of us at one point. Then guidelines recommend maximizing the dose till you see benefit without running into side effects. One of the parts of health care that I disagree with on many levels.
Wasn't there an old conspiracy theorist thread on the old platform? Did it get deleted?Anyone ready for me to merge this with the TAY thread?
Let me get this straight, we're using Wikipedia, an open platform that anyone can edit as evidence, yet a licensed doctor and biophysicist who gives a thorough dissertation on her stance is not addressed? Mind you this physician has gave her stance on a multitude of levels where no has been able to refute what she says. I considered this before I even posted the link but I honestly didn't think you would really use wikipedia as a reference.
.png")
I don't think you fully grasp how Wikipedia works.
In an academic setting, Wikipedia would not be an appropriate source. But the articles cited in the wiki article would. Just editing a wiki page and take a snip of it doesn't just "change the narrative"
Did I say it was bad to go to a doctor or noWhen one of your kids are sick, who do you seek help from?
Your local Youtube conspiracy theorist?