- 5,372
- 4,423
- Joined
- Sep 18, 2013
All that is cool and I 100 percent agree with you. I’m ignorant to HIV but.............Another physician checking in. This thread reaks of the flat-earther and nut-job conspiracy mongers and millenial pseudo-philosophers. Please don't think that going to a top 10 school and taking "some pre-med classes" before failing organic chemistry and not getting into med school makes you somehow an expert in the field of virology.
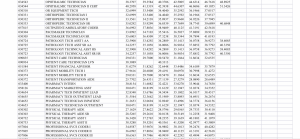
Source: UpToDate (most widely used evidence based resource used by physicians in practice today)
The natural history and clinical features of HIV infection in adults and adolescents
Author:
Paul E Sax, MD
Section Editor:
Martin S Hirsch, MD
Deputy Editor:
Allyson Bloom, MD
All topics are updated as new evidence becomes available and our peer review process is complete.
Literature review current through: Nov 2018. | This topic last updated: Jul 24, 2018.
INTRODUCTION — Since the original description in 1981 of an unusual cluster of cases of Pneumocystis carinii pneumonia and Kaposi sarcoma in previously healthy men who have sex with men, substantial advances in our understanding of the acquired immunodeficiency syndrome (AIDS) have been achieved. The identification of a cytopathic retrovirus in 1983 and development of a diagnostic serologic test for human immunodeficiency virus (HIV) in 1985 have served as the basis for developing improvements in diagnosis.
In addition, therapy was dramatically altered with the introduction of antiretroviral drugs in 1987 and revolutionized by combination antiretroviral therapy (ART) in 1996. In the three years following the introduction of effective ART, mortality, AIDS, AIDS-defining diagnoses, and hospitalizations all decreased 60 to 80 percent. The EuroSIDA study, comparing this early ART period with pre-ART and later ART (1998 to 2002) treatment periods, found a sustained decrease in mortality and progression to AIDS with ongoing ART [1]. Despite the absence of a cure, the natural history of the disease was radically changed, and now, certain patients with HIV infection without other significant comorbidities who are treated before significant immunosuppression can expect a life expectancy approaching that of the general population [2].
Despite these advances, it is still useful to review the natural history of HIV infection without ART and the classification of disease. Although modified from the initial case definition, the newer Centers for Disease Control and Prevention (CDC) classification system remains the cornerstone for diagnosing HIV and AIDS.
This topic reviews the case definition, stages, and natural history of HIV infection. The epidemiology of HIV infection, factors that influence the natural history of HIV infection, and the impact of ART on the natural history are discussed elsewhere. (See "Global epidemiology of HIV infection" and "Use and impact of antiretroviral therapy for HIV infection in resource-limited settings".)
CASE DEFINITION — Clarification of the case definition of HIV infection is important for surveillance and public health purposes. Organizations such as the Centers for Disease Control and Prevention (CDC) in the United States and the World Health Organization (WHO) have established case definitions to standardize the description of HIV infection cases. Although they reflect the clinical diagnostic evaluation for HIV infection, these case definitions are not intended to serve as the bases for clinical decisions in individual patients. The clinical diagnosis of HIV infection is discussed in detail elsewhere. (See "Screening and diagnostic testing for HIV infection", section on 'Testing algorithm'.)
CDC classification — The CDC laboratory criteria for the case definition of HIV infection include a positive result on a multitest algorithm (eg, a positive result on an antibody or combined antibody/antigen assay and a positive test on a supplemental test distinct from the first) or a positive HIV virologic test (table 1) [3]. This case definition is inclusive of testing algorithms that do not incorporate Western blot or immunofluorescent assays. In the United States, all HIV infections can be assumed to be with type 1 (HIV-1) unless specific testing has demonstrated infection with type 2 (HIV-2) or cannot distinguish the type. (See 'HIV-2 infection' below.)
The CDC case definition also classifies HIV infection based on the absolute CD4 cell count as stage 1 (CD4 cell count >500 cells/microL), 2 (CD4 cell count 200 to 499), or 3 (CD4 cell count <200 cells/microL). Criteria for stage 3 are also met by the presence of a stage 3 (ie, AIDS)-defining opportunistic illness (table 2). The classification system also includes stage 0 infection, which is defined as early infection (with a negative or indeterminate HIV test within 180 days prior to the first confirmed positive test) regardless of the CD4 cell count or presence of opportunistic illness.
WHO classification — The WHO case definition of HIV infection includes 1) a positive result on a HIV antibody test confirmed by a positive result on a second, different HIV antibody test and/or 2) a positive virologic test confirmed by a second virologic test [4]. The WHO classification system for staging established HIV infection uses both immunologic (table 3) or clinical (table 4) criteria.
OVERVIEW OF STAGES OF HIV INFECTION — HIV infection can be divided into the following stages:
●Viral transmission. (See 'Viral transmission' below.)
●Acute HIV infection (also called primary HIV infection or acute seroconversion syndrome, among other terms). (See 'Acute and early HIV infection' below.)
•Seroconversion describes the development of detectable antibodies, which generally occurs within the first several weeks after infection (depending on the antibody test used).
●Chronic HIV infection. (See 'Chronic HIV infection, without AIDS' below and 'AIDS and advanced HIV infection' below.)
•Asymptomatic.
•Early symptomatic HIV infection (previously known as AIDS-related complex [ARC] or Class B).
•AIDS characterized by a CD4 cell count <200 cells/microL or the presence of any AIDS-defining condition (table 5).
•Advanced HIV infection characterized by a CD4 cell count <50 cells/microL
VIRAL TRANSMISSION
Mode of acquisition — HIV infection is usually acquired through sexual intercourse, exposure to infected blood, or perinatal transmission. The mode of acquiring HIV infection was undetermined in 4 percent of the cases originally reported to the United States Centers for Disease Control and Prevention (CDC). A careful review of 32,497 cases, however, revealed that only 0.2 percent had no clearly defined risk factor.
The distribution of the modes of transmission of HIV infection varies in different countries. In resource-limited areas, vaginal sex is responsible for 70 to 80 percent of HIV infections, and perinatal transmission and injection drug use (IDU) for 5 to 10 percent each [5]. By contrast, in the United States and Western and Central Europe, male-to-male sexual contact is the most common route of HIV transmission. (See "Global epidemiology of HIV infection", section on 'Modes of transmission driving the epidemic'.)
Risk factors — Risk factors for HIV transmission include high viral load, certain sexual behaviors, presence of ulcerative sexually transmitted infections (STIs), and lack of circumcision, as well as certain host and genetic factors [6-8]. (See "HIV infection: Risk factors and prevention strategies", section on 'Risk factors for infection'.)
●Viral load – For all modes of transmission, a higher viral load is associated with a greater risk of transmission. This is reflected in models that suggest that a large proportion of HIV infections are transmitted by individuals with acute and early infection, a finding likely related to the high levels of viremia that are seen in the setting of acute infection [9]. (See "Acute and early HIV infection: Clinical manifestations and diagnosis" and "Acute and early HIV infection: Clinical manifestations and diagnosis", section on 'HIV RNA detection'.)
●Sexual behavior – The type of sexual exposure (eg, receptive anal intercourse versus receptive vaginal intercourse) and whether it was protected with condoms or not affects the risk of HIV transmission. In addition, other factors, such as the number of sexual partners or sex under the influence of recreational drugs also affect the risk. As an example, in a study of 3257 men who have sex with men (MSM) in six United States cities, risk factors for HIV acquisition included history of a large number of sexual partners, unprotected receptive anal sex with a partner with an unknown HIV serostatus, and use of nitrate inhalants [10].
●Sexually transmitted infections – The presence of other STIs also increases the risk of HIV acquisition, as demonstrated in a study of 174 monogamous Ugandan couples with discordant HIV serostatus [9,11]. The probability of transmission was approximately four times higher in patients with genital ulceration compared with those without. Multiple other studies have confirmed these results. (See "Epidemiology, clinical manifestations, and diagnosis of genital herpes simplex virus infection", section on 'HSV-2 and risk of HIV transmission' and "Syphilis in the HIV-infected patient", section on 'Epidemiology'.)
●Lack of circumcision – Several randomized trials have demonstrated a decreased risk of HIV acquisition with circumcision in heterosexual men [12-15]. In addition, lack of circumcision has been associated with risk of HIV transmission in cohorts of heterosexual couples and MSM [16].
●Genetic background – Similarity of human leukocyte antigen (HLA) class I alleles between HIV discordant couples may affect the risk of transmission (see "Human leukocyte antigens (HLA): A roadmap") by selecting for viral strains that are more likely to escape the immune containment of the uninfected partner. In a study of 125 initially serodiscordant couples with intracouple transmission, and 104 persistently serodiscordant couples, sharing of HLA-B alleles was associated with accelerated intracouple transmission of HIV after controlling for other variables (hazard ratio
The earth is flat